



Red light and near-infrared exposure and skin pigmentation
So recently I saw a reel that said red light and near-infrared exposure can cause pigmentation. So I went digging to answer the question.
So can it cause pigmentation? The short answer is yes, red light and near-infrared can worsen pigmentation in some circumstances, but the main culprit is usually not the wavelength by itself.
The better reading of the literature is that pure, narrow-band, non-thermal red light in the 630–660 nm range has little evidence of directly causing hyperpigmentation in normal skin, and some red and NIR photobiomodulation studies actually show reduced melanogenesis. By contrast, heat-generating or cumulative exposures in the red/NIR range can plausibly worsen pigmentation through thermal stress, inflammatory signalling, oxidative stress, vascular changes, and barrier disruption, especially in melasma, post-inflammatory hyperpigmentation, rosacea, and darker Fitzpatrick phototypes.
The most important distinction is non-thermal photobiomodulation versus photothermal heating. A 630 nm human study found no hyperpigmentation at the red end of the visible spectrum, whereas blue-violet light did darken skin; 660 nm, 830 nm, and 850 nm studies reported anti-melanogenic effects in vitro and/or ex vivo. On the other hand, repeated heat exposure around 40–42°C can increase melanocyte dendricity, tyrosinase-related markers, and keratinocyte-driven melanogenesis and can amplify UVB-driven pigmentation. Chronic infrared heat exposure is also well known to cause erythema ab igne, a reticulated hyperpigmented dermatosis.
Clinically, the highest-risk scenarios are not usually a properly designed red LED panel used conservatively. The higher-risk scenarios are broad thermal infrared sources such as saunas, incandescent/infrared lamps, heating pads, and high-cumulative-fluence or multi-pass NIR laser exposure that warms tissue or disrupts the barrier. In melasma, repeated 1064 nm Nd:YAG treatment has been linked to melanocyte activation and increased transepidermal water loss, even when pigment initially improves, which may help explain relapse.
For practical use, the safest default for pigment-prone people is: prefer narrow-band, low-heat devices; avoid “warming” the skin; keep sessions conservative; patch test; cool the skin if needed; and stop immediately if sessions cause prolonged warmth, flushing, or delayed darkening. People with melasma, PIH, rosacea, or Fitzpatrick IV–VI should use a particularly low-and-slow approach or avoid heat-heavy red/NIR devices entirely.
What the evidence says
The strongest direct human evidence against a major intrinsic pro-pigmenting effect of red light itself comes from Duteil et al. (2014) in Pigment Cell & Melanoma Research. In that clinical and histological study, 415 nm blue-violet light induced hyperpigmentation, but 630 nm red light did not induce hyperpigmentation, even at the highest investigated dose reported in later reviews as 150 J/cm². That is an important anchor point: if a narrow-band red exposure is kept non-thermal, the available human evidence does not support red light behaving like UV or blue-violet visible light.
That said, red and NIR are not biologically inert. Depending on context, they can alter nitric oxide signalling, mitochondrial activity, reactive oxygen species, cytokines, growth factors, melanocyte migration, and vascular tone. The dermatology PBM reviews in JAAD define photobiomodulation as light use in the 620–700 nm red and 700–1440 nm NIR ranges and emphasise a biphasic dose response: dose, irradiance, fluence, repetition, and treatment regimen change the biological outcome. In plain English, the same nominal wavelength can help, do nothing, or irritate, depending on how hard and how often it is delivered.
Recent primary work also cuts against the simplistic idea that NIR is uniformly pigment-provoking. Kim et al. (2012), in Acta Dermato-Venereologica, found that 830 nm LED exposure at 1–20 J/cm² and 850 nm at 1 J/cm² reduced melanin production and tyrosinase expression in human melanocytes and three-dimensional culture models. More recently, Dan et al. 2024 in Pigment Cell & Melanoma Research reported that an 830 nm LED at 5–20 J/cm² inhibited melanogenesis via FOXO3a and reduced epidermal basal pigmentation in an ex vivo human skin model.
A similar anti-melanogenic signal has also been reported in the red band. Oh et al. (2017), in Photodermatology, Photoimmunology & Photomedicine, found that 660 nm LED inhibited melanogenesis in in vitro and in vivo models. So, if the question is “does red/NIR always darken skin?”, the answer is plainly no. Under several PBM-style conditions, the opposite has been observed.
The part that pushes risk upward is heat. Nakazawa et al. (1998) in the Journal of Investigative Dermatology, exposed melanocytes and skin-equivalent systems to 42°C for 1 hour and found increased dendricity, increased tyrosinase activity per cell, and more dopa-positive and TRP-1-positive melanocytes after repeated heat exposure. Gu et al. (2014) in Archives of Dermatological Research refined that picture: 40°C for 1 hour over 5 days promoted melanocyte differentiation signals and, crucially, had an additive effect on UVB-induced tyrosinase activation and melanogenesis. That matters because most people are not exposed to light in a vacuum; they are exposed to UV, visible light, hot rooms, physical activity, or skin irritation layered on top.
The newest mechanistic heat study goes further. Zhang et al. (2023) in iScience, reported that human foreskin tissue exposed to 41°C developed significant pigmentation and that heat promoted melanogenesis by increasing keratinocyte paracrine signalling through the TRPV3/Ca²⁺/Hedgehog pathway. This is a good reminder that pigment worsening in real skin is often not just "melanocytes absorb photons and make pigment”. It can be keratinocyte-driven, inflammatory, hormonal, or vascular, with the whole skin microenvironment involved.
Qualitative risk map by wavelength and source
| Exposure scenario | Direct melanogenic evidence | Heat burden | Overall concern for worsening pigmentation |
|---|---|---|---|
| 630 nm narrow-band red LED, skin stays cool | Human study found no hyperpigmentation | Low | Low |
| 660 nm red LED PBM | Inhibitory melanogenesis signals in preclinical models | Low if truly PBM | Low |
| 830–850 nm narrow-band NIR LED PBM | Anti-melanogenic in several preclinical models | Low to moderate, device-dependent | Low to low-moderate |
| 1064 nm low-fluence medical laser, tightly controlled | Can reduce melanin via non-thermal biomodulation | Moderate if settings drift upwards. | Low-moderate |
| 1064 nm cumulative / multi-pass / hotter settings | Barrier injury, inflammation, relapse risk in melasma | Moderate to high | Moderate to high |
| Infrared saunas, incandescent IR lamps, heating pads, broad heat sources | Mostly indirect evidence via thermal injury, rosacea provocation, erythema ab igne | High | High in susceptible skin |
Mechanisms that can worsen pigmentation
Photobiomodulation does not act through just one switch. In red and NIR ranges, cytochrome c oxidase, nitric oxide biology, mitochondrial signalling, and low-level reactive oxygen species are commonly invoked, and the response is typically hormetic or biphasic. At suitable doses this can be reparative or anti-inflammatory, but once irradiance, cumulative exposure, or heat climbs too high, signalling can flip from adaptive to irritating.
There is also evidence that red light can stimulate melanocyte behaviour in some disease contexts. Yu et al. (2003), in the Journal of Investigative Dermatology, showed that a 632.8 nm He-Ne laser increased growth factor release from keratinocytes/fibroblasts, enhanced melanocyte migration and proliferation, and promoted repigmentation in segmental vitiligo. Lan et al. (2009), in the British Journal of Dermatology, likewise reported melanocyte proliferation via mitochondria-related pathways. Those are not hyperpigmentation trials, but they do show that red light can activate melanocyte biology under some conditions, which is why “red light is always pigment-neutral” is too simplistic.
Heat-driven pathways are more worrying for pigment worsening than photon-driven red-light pathways. Heat activates TRP channels, especially TRPV1 and TRPV3, triggers calcium signalling, and can increase inflammatory mediators and matrix remodelling. Li et al. showed that heat-shock-induced MMP-1 expression in human keratinocytes is mediated by TRPV1 and calcium-dependent signalling. Schieke et al. (2002), in JID, showed that infrared-A can induce MMP-1 through ERK1/2 and notably found that this was not mediated by heat-shock protein 70 under the tested conditions, implying that classical heat-shock proteins are part of the thermal-stress landscape but are not the sole or necessary route to downstream skin change.
Oxidative stress is another credible bridge between NIR/infrared exposure and pigment worsening. Schroeder et al. 2008 in JID found that physiologically relevant infrared- A exposure in vivo increased dermal MMP-1 in most subjects and reduced skin antioxidant content, while antioxidants prevented IRA-induced MMP-1 expression. The 2023 review by Horton et al. in Photodermatology, Photoimmunology & Photomedicine similarly summarised that IR can increase ROS and photoageing signals while also noting that the literature is mixed and not fully standardised. Oxidative stress matters because melanogenesis itself is a redox-sensitive process.
Nitric oxide and vascular signalling are relevant too, but the data are mixed. Antioxidants 2024 reported that 660 nm and 850 nm increased NO release in cultured keratinocytes/fibroblasts, whereas Hazell et al. (2026) in Antioxidants found that daylight-equivalent broad-spectrum red, including infrared, did not significantly increase NO release in their low-level exposure model. That discrepancy is important: it suggests that narrow-band clinical PBM exposures and low-level ambient red/NIR exposures are not biologically equivalent. NO can be helpful, neutral, or inflammation-linked depending on level, cell type, and context.
Vascular and inflammatory pathways also intersect with melasma and rosacea. Melasma is increasingly understood as a disorder involving pigmentation, inflammation, mast cells, vascularity, and barrier dysfunction, not just excess pigment. Rosacea can be provoked by infrared heat alone, independent of UV, with significant vasodilation. In people with heat-sensitive rosacea or inflammatory pigmentary disorders, repeated warming may therefore worsen erythema first and pigmentation secondarily, especially when the barrier is already compromised.

The flowchart above reflects the best-supported synthesis of the current literature: non-thermal PBM can be neutral or anti-melanogenic, whereas heat-heavy or inflammatory exposures can push the skin towards pigment worsening.
Evidence by wavelength, dose, frequency, and device
The dose issue matters as much as the wavelength issue. In the accessible melanogenesis literature, the “safe/neutral or inhibitory” red/NIR studies cluster around modest fluences such as 1–20 J/cm² in cell/ex vivo work, while much higher red-light safety studies escalate to 160–640 J/cm² on healthy human skin. A phase I red-light safety programme later concluded that high-fluence red LED light was safe up to 320 J/cm² in skin of colour and 480 J/cm² in non-Hispanic Caucasian individuals, implying skin type can affect tolerance even when pigmentation outcomes are not the endpoint. That does not mean 320 J/cm² is a good home-use target; it means pushing the dose upward is not pigment-neutral simply because the wavelength is “red”.
Medical 1064 nm laser literature illustrates the central thermal point very clearly. Dong et al. (2025) showed that a 1.0 J/cm², 2-pass low-fluence 1064 nm treatment could suppress melanogenesis through non-thermal biomodulation, whereas more passes or higher cumulative delivery caused a measurable temperature rise, cytoskeletal injury, and viability loss. At the same time, Gao et al. (2019) found that in actual melasma patients treated with 1064 nm Nd:YAG for 10 sessions, the melanin index fell, but dendritic melanocyte activation and TEWL increased, and higher TEWL was associated with relapse. This is exactly why “NIR helped melasma in one study” and “NIR worsened pigmentation in another” can both be true: the protocol and tissue response are different.
Broad heat sources are a separate category. Infrared saunas use infrared wavelengths rather than simple hot air, with near-infrared saunas occupying roughly the 0.7–1.4 µm band. Incandescent bulbs and therapeutic IR lamps are broadband thermal emitters, not narrow-band PBM sources; standard incandescent bulbs convert most input energy into heat or infrared rather than visible light, and some IR heating lamps show a pronounced output peak near 1000 nm. For pigment-prone patients, those sources should be thought of as heat devices first and light devices second.
Key study comparison
Quality below is a pragmatic assessment of directness and design, not a formal GRADE rating.
| Study | Wavelength / source | Dose, temperature, or schedule | Population / model | Pigment outcome | Quality |
|---|---|---|---|---|---|
| Duteil et al., 2014, Pigment Cell Melanoma Research, DOI 10.1111/pcmr.12273 | 415 nm vs 630 nm LED | Increasing doses; later reviews state red tested up to 150 J/cm² | Healthy volunteers, skin types III–IV | 630 nm did not induce hyperpigmentation; 415 nm did | Moderate-high direct human evidence |
| Nakazawa et al., 1998, J Invest Dermatol, DOI 10.1046/j.1523-1747.1998.00204.x | Heat | 42°C for 1 h, repeated over days | Human melanocytes, coculture, skin equivalents | Increased melanocyte dendricity, tyrosinase activity, dopa/TRP-1 positive cells | Moderate mechanistic relevance |
| Gu et al., 2014, Arch Dermatol Res, DOI 10.1007/s00403-014-1461-y | Heat ± UVB | 40°C for 1 h for 5 days; UVB 20 mJ/cm² for 5 days | Human epidermal melanocytes, phototype III | Heat alone altered differentiation signalling; additive with UVB for tyrosinase and melanogenesis | Moderate |
| Zhang et al., 2023, iScience, DOI 10.1016/j.isci.2023.106749 | Heat stress | 41°C | Human foreskin tissue; keratinocyte–pigment cell models | Significant pigmentation via TRPV3/Ca²⁺/Hh keratinocyte paracrine pathway | Moderate |
| Kim et al., 2012, Acta Derm Venereol, DOI 10.2340/00015555-1319 | 830 nm, 850 nm LED | 830 nm 1–20 J/cm²; 850 nm 1 J/cm² | Human melanocytes; 3D culture | Reduced melanin production and tyrosinase expression | Moderate |
| Oh et al., 2017, Photodermatol Photoimmunol Photomed, DOI 10.1111/phpp.12276 | 660 nm LED | Dose details not fully surfaced in accessible abstract metadata | In vitro and in vivo melanogenesis models | Inhibitory effect on melanogenesis | Moderate, though accessible dosing detail is incomplete |
| Yu et al., 2003, J Invest Dermatol, DOI 10.1046/j.1523-1747.2003.12011.x | 632.8 nm He-Ne laser | Keratinocyte/fibroblast irradiation 0.5–1.5 J/cm²; vitiligo treatment 3.0 J/cm² once or twice weekly | In vitro melanocyte biology + segmental vitiligo patients | Stimulated melanocyte migration/proliferation and repigmentation | Moderate for melanocyte activation, indirect for hyperpigmentation risk |
| Gao et al., 2019, Lasers in Medical Science, DOI 10.1007/s10103-018-2658-7 | 1064 nm Q-switched Nd:YAG | 10 treatments | 25 female melasma patients | Initial pigment reduction but melanocyte activation, higher TEWL, relapse association | Moderate-high clinical relevance |
| Dong et al., 2025, Lasers in Medical Science, DOI 10.1007/s10103-025-04702-6 | 1064 nm low-fluence Q-switched Nd:YAG | Non-thermal at 0.5–2.0 J/cm², 2-pass; higher passes increased temperature | B16F10 cells, mice, macrophage models | Low-fluence settings suppressed melanogenesis; higher cumulative settings caused thermal effects | Moderate |
| Schroeder et al., 2008, J Invest Dermatol, DOI 10.1038/jid.2008.116 | Infrared-A 760–1440 nm | Physiologically relevant in vivo IRA doses | Healthy human skin in vivo | Increased dermal MMP-1 and reduced antioxidants; antioxidants prevented the MMP-1 response | Moderate indirect evidence for heat/oxidative risk |
Who is most at risk
The people most likely to have trouble are those with a pigmentary disorder already in play or with high inflammatory reactivity. Melasma is the standout group. Modern melasma reviews describe it as a chronic disorder involving pigment, vascularity, mast cells, inflammation, and barrier dysfunction, and not simply a UV-induced brown patch problem. That means a device that warms the skin, causes repeated erythema, or subtly disrupts the barrier may worsen a melasma-prone phenotype even if the wavelength itself is not strongly melanogenic.
Post-inflammatory hyperpigmentation is another high-risk setting, especially in skin of colour. Reviews and complication papers consistently note that higher Fitzpatrick phototypes have a higher risk of pigmentary sequelae from lasers and energy-based devices, and PIH is especially common and stubborn in phototypes III–VI. For that reason alone, any red/NIR device that causes repeated flushing, blistering, abrasion, or delayed irritation should be treated as a pigment risk in darker phototypes, even if the marketing says “non-invasive” or “safe for all skin tones".
Rosacea matters because it is a heat-sensitive, vasodilatory, inflammatory condition. In a 2023 JAAD study, infrared heat alone could provoke rosacea via significant blood-flow-mediated vasodilation, independent of ultraviolet exposure. Rosacea does not always equal hyperpigmentation, but it does mean that heat-heavy red/NIR treatments can create a persistently inflamed background in which post-inflammatory darkening is more likely, especially in melanocompetent skin.
The biggest confounders are the obvious ones and the ones people forget. UV exposure, blue/visible light; recent actives such as retinoids or exfoliating acids; friction; occlusion; hot showers or exercise immediately before a session; and barrier impairment can all move the skin closer to a pro-inflammatory, pro-pigment state. Hormonal factors matter particularly in melasma. So when someone says a “red light mask caused pigmentation", the right analytic question is not only "What wavelength was it?” but also "How hot did it get, what else was on the skin, and what background disease was already present?”
Practical recommendations for clinic and home use
If the goal is to minimise pigment risk, the safest device choice is usually a narrow-band red LED device in the 630–660 nm range that does not noticeably warm the skin, rather than a heat-heavy mixed-spectrum device. Narrow-band 830–850 nm NIR devices can also be reasonable, but I would be stricter with them because NIR carries more thermal potential than visible red, and consumer devices vary wildly in actual output. I would be most cautious with broadband IR lamps, infrared saunas, heating pads, close-contact masks that trap heat, and repeated 1064 nm laser exposure unless there is a strong medical reason and good clinician oversight.
A sensible device-selection checklist is brief. Look for a device that clearly discloses peak wavelengths, irradiance at a stated distance, a session timer, and whether the source is a narrow-band LED/laser or broad thermal IR. Avoid devices that also emit UV or strong blue light unless those wavelengths are deliberately indicated for another reason. A pigment-prone user should strongly prefer a device that does not leave the skin feeling hot and should treat “warming” as a warning sign, not a bonus feature. That recommendation is a synthesis from the PBM dosing literature plus the heat/pigment papers, rather than a single formal guideline.
A conservative monitoring protocol is worth the effort. Start with a test area or a short facial session. Take baseline photographs in the same light, and document any pre-existing melasma, PIH, flushing, or irritation. For the first two weeks, reassess at 24 hours and 72 hours after each session. If you see persistent warmth, erythema lasting beyond a day, stinging, new roughness, or delayed darkening, stop. In a clinic, add melanin/erythema measurements if available. This is an inference from the melasma relapse, thermal injury, and complication literature; it is conservative because the home-use evidence base is still thin.
For session limits, the safest principle is the minimum effective dose. In people with melasma, PIH, rosacea, or Fitzpatrick IV–VI, it is harder to justify long sessions, stacked passes, or daily high-output use. The cumulative-exposure lesson from the 1064 nm work is that a setting that is non-thermal in one pass can become thermal when repeated. For home users, a cautious starting point is to use the manufacturer’s lowest reasonable programme and not escalate based on impatience. If the skin feels meaningfully warmer after treatment, the session was probably too aggressive for a pigment-risk profile.
Mitigation strategies are sensible but should be understood honestly. Cooling is logical because the risk signal in the literature tracks with thermal load. Topical antioxidants are also biologically plausible because infrared- A study showed oxidative pathways and MMP-1 induction, and antioxidants prevented IRA-induced MMP-1 expression in vivo in one classic human skin study. What is not yet well proven is that antioxidants specifically prevent red/NIR-induced pigment worsening in routine home use. So I would describe antioxidants and cooling as reasonable risk reducers, not guaranteed fixes.
For patients with melasma, strict overall photoprotection remains essential even if the device itself emits no UV. The broader melasma literature continues to support comprehensive UV and visible-light protection, including tinted sunscreens where appropriate, because concurrent daylight exposure can make any heat or inflammation problem worse. A red/NIR treatment plan that ignores ambient UV/visible light is incomplete.
Open questions and research needs
The biggest gap is the lack of high-quality human trials that isolate red or 700–1100 nm NIR exposure as the sole variable and then measure pigmentation outcomes, especially in melasma, PIH, rosacea, and Fitzpatrick IV–VI skin. Most of the literature is either mechanistic, mixed-indication clinical work, or studies designed for wound healing, fibrosis, or melasma treatment rather than for adverse pigmentation surveillance.
Another major problem is poor dosimetry standardisation. Many publications and device listings do not report enough detail on irradiance, distance, duty cycle, cumulative fluence, pass number, skin-surface temperature, or spectral purity to let clinicians translate findings cleanly into real-world advice. This is especially messy in consumer devices and mixed red/NIR products.
Data are also thin in the 900–1100 nm range, apart from broad infrared-A and 1064 nm medical laser work. Most melanogenesis papers cluster around 630–660 nm, 830–850 nm, and 1064 nm, which means there is still a genuine knowledge gap in much of the user-specified NIR band.
The overall conclusion, then, is red light and NIR do not appear to be major direct pigment drivers in the way UV and blue-violet light are, but they absolutely can worsen pigmentation when they act as heat, inflammatory, or barrier-disrupting exposures. If you keep the skin cool, keep the dose conservative, and respect susceptibility factors, the risk falls sharply. If the device behaves like a heat source, the risk rises sharply.
Author
Through Roccoco Botanicals, Jacine has trained skin professionals globally and developed award-winning formulations used in clinics across Australia, the USA, Canada, and New Zealand. Her writing focuses on translating complex skin science into practical, evidence-based education that empowers both practitioners and consumers to make informed decisions about skin health.
https://www.cidjournal.com/article/S0738-081X%2823%2900168-2/fulltext
https://europepmc.org/article/MED/24888214
https://link.springer.com/article/10.1007/s10103-024-04100-4
https://www.sciencedirect.com/science/article/abs/pii/S0190962224001865
https://www.medicaljournals.se/acta/content/abstract/10.2340/00015555-1319
https://www.x-mol.com/paper/1212910884416725002
https://www.sciencedirect.com/science/article/pii/S0022202X15401174
https://pmc.ncbi.nlm.nih.gov/articles/PMC10192915/
https://link.springer.com/article/10.1007/s10103-025-04702-6
https://link.springer.com/content/pdf/10.1007/s10103-018-2658-7.pdf
https://www.sciencedirect.com/science/article/pii/S0022202X15301184
https://www.sciencedirect.com/science/article/pii/S0022202X15331420
https://www.sciencedirect.com/science/article/pii/S0022202X15336241
https://www.mdpi.com/2076-3921/13/10/1176
https://www.sciencedirect.com/science/article/abs/pii/S0190962223028505
https://escholarship.org/uc/item/79v4019x
https://link.springer.com/article/10.1007/s00403-014-1461-y
https://www.em-consulte.com/article/1637920/heat-stimuli-test-by-infrared-reveals-rosacea-as-a
https://link.springer.com/article/10.1007/s40257-024-00863-2
https://link.springer.com/article/10.1007/s44411-025-00272-9
Read more

There is a point many women reach, usually somewhere in their forties or fifties, where their skin simply stops behaving the way it used to. Products that worked reliably for years start to feel wr...
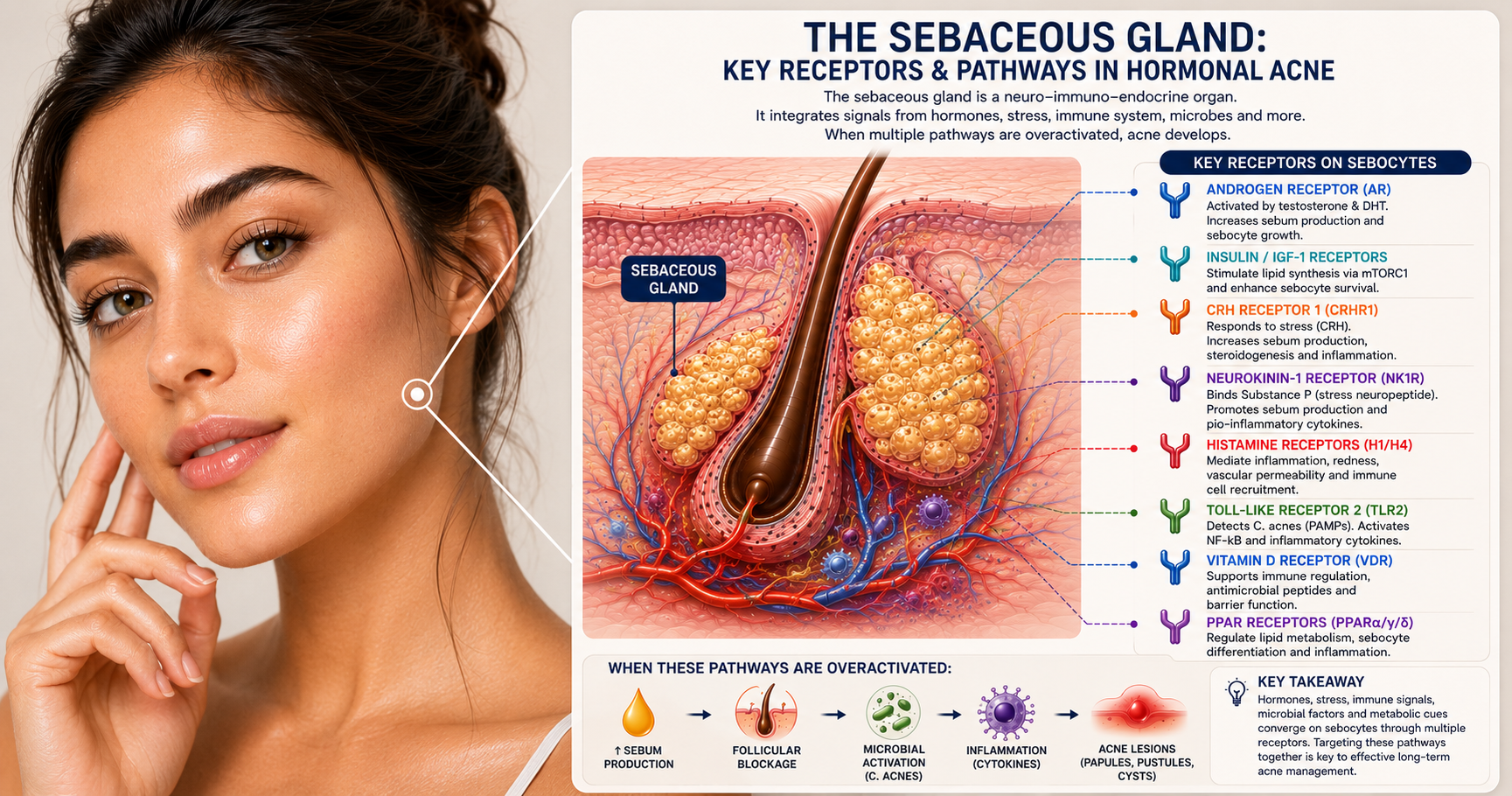
For years, hormonal acne has been blamed on hormones alone. But modern science tells a far more complex story. Discover how your sebaceous glands act as neuro-immuno-endocrine organs, responding to...